2025 Behavioral Health Crisis Response Team Annual Report
Executive Summary
This report is a summary of the Behavioral Health Crisis Response Team’s (BHCRT) operations from January 1, 2025, through December 31, 2025.1The team provides crisis intervention, assessment, de-escalation and referral to services. Clinicians are dispatched via Boulder Police and Fire Communications to respond with or without the Boulder Police Department for calls that have a behavioral health component. Clinicians co-respond with police on calls for service that involve more dynamic situations, while alternative response focuses on lower acuity calls that do not require police response. The alternative response option was paused on August 28, 2025, but the team plans to relaunch an alternative response in the second half of 2026.
Highlights of 2025 include:
BHCRT responded to 1,479 calls for service, 248 information calls and 638 follow ups.
Case managers had 729 contacts, fewer than in previous years. This reflects decreased staffing from 2024 to 2025.
Demand data indicate that overall BHCRT program hours are well matched to hours when the service is needed in the community.
About 1 in 5 BHCRT encounters involved a person experiencing homelessness. Another 6.1% (36) involved an individual at risk of losing housing.
BHCRT interacted with 819 distinct clients in 2025. This total does not include clients who asked to remain anonymous. 222 (27.1%) distinct clients had more than one encounter with BHCRT, with 10 clients interacting with the BHCRT an average of 14.8 times in 2025.
BHCRT clinicians initiated emergency mental health holds 43 times (2.9% of calls) in 2025. One of the benefits of BHCRT clinical expertise on behavioral health calls is the reduction of unnecessary involuntary treatment, which lessens negative impacts to people by preserving their autonomy, and reduces avoidable utilization of Emergency Medical Services (EMS) and emergency departments.
Of the 1,479 BHCRT calls for service the team responded to in 2025, five (0.3%) involved use of force by an officer.
24 (1.6%) of BHCRT’s calls for service in 2025 involved an arrest.
BHCRT facilitated return of Fire/EMS to service 170 times (40.3% of applicable interactions).
BHCRT facilitated return of police to service 515 times (45.7% of applicable interactions).
Who Does BHCRT Serve?
The BHCRT assists a wide variety of people in the City of Boulder.
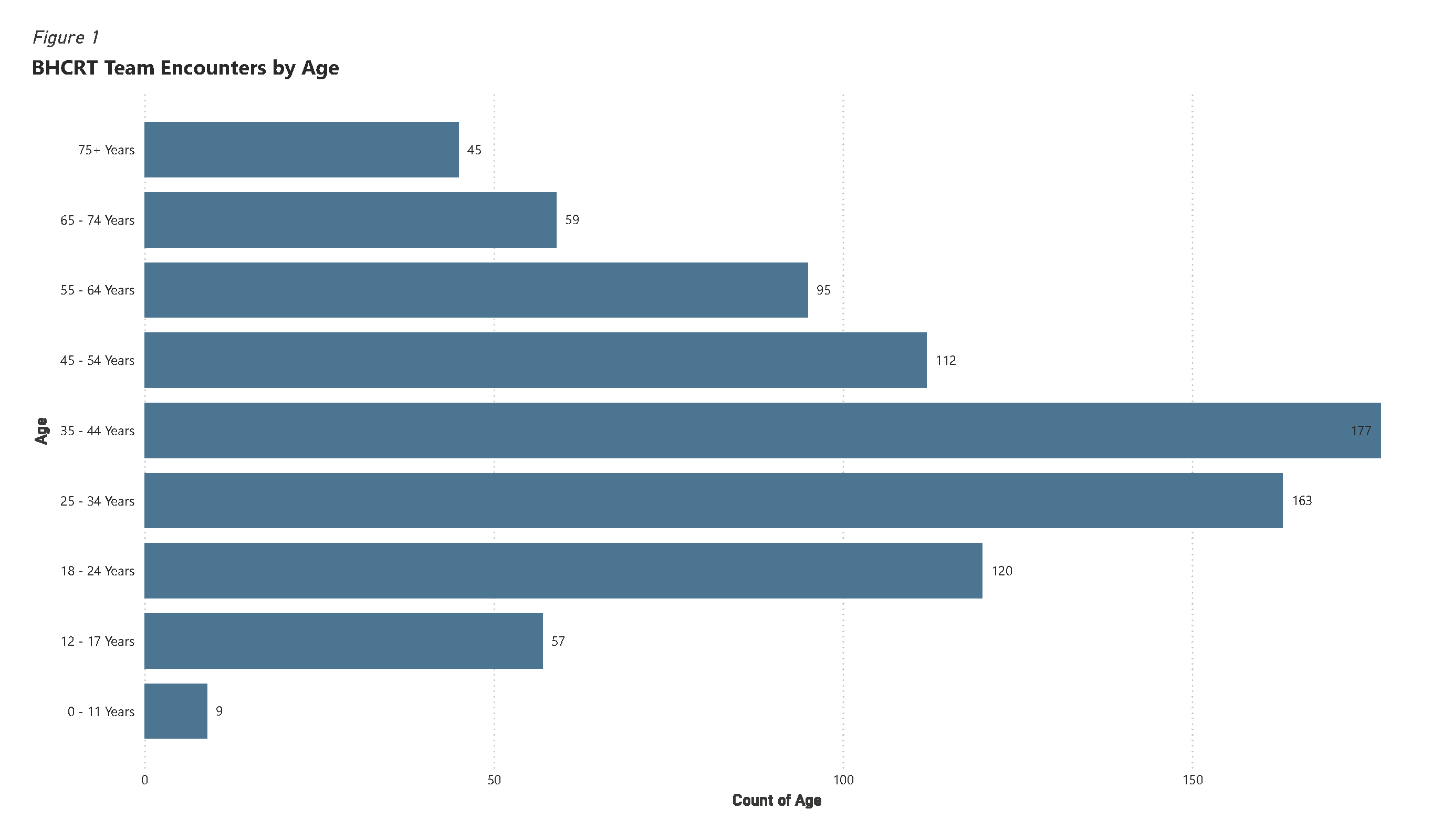
Age
The median age of BHCRT clients in 2025 was 38 years old, with a range from 6 to 97 years old.
Figure 1: BHCRT Encounters by Age
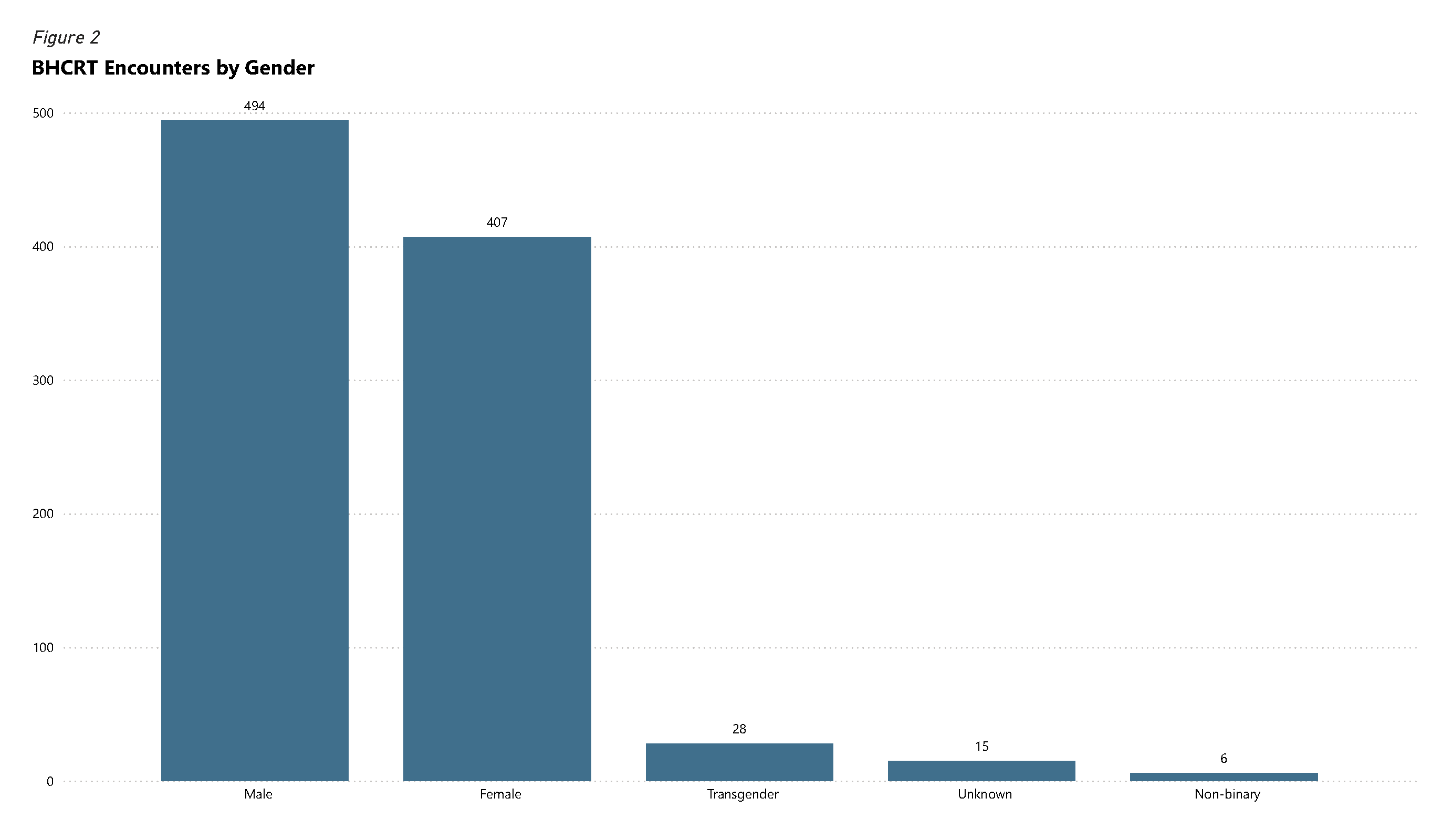
Gender
Of the 950 unique clients who reported their gender, 52.0% identified as male, 42.8% as female, 2.9% as transgender, 0.6% as non-binary and 1.6% were unknown.
Figure 2: BHCRT Encounters by Gender
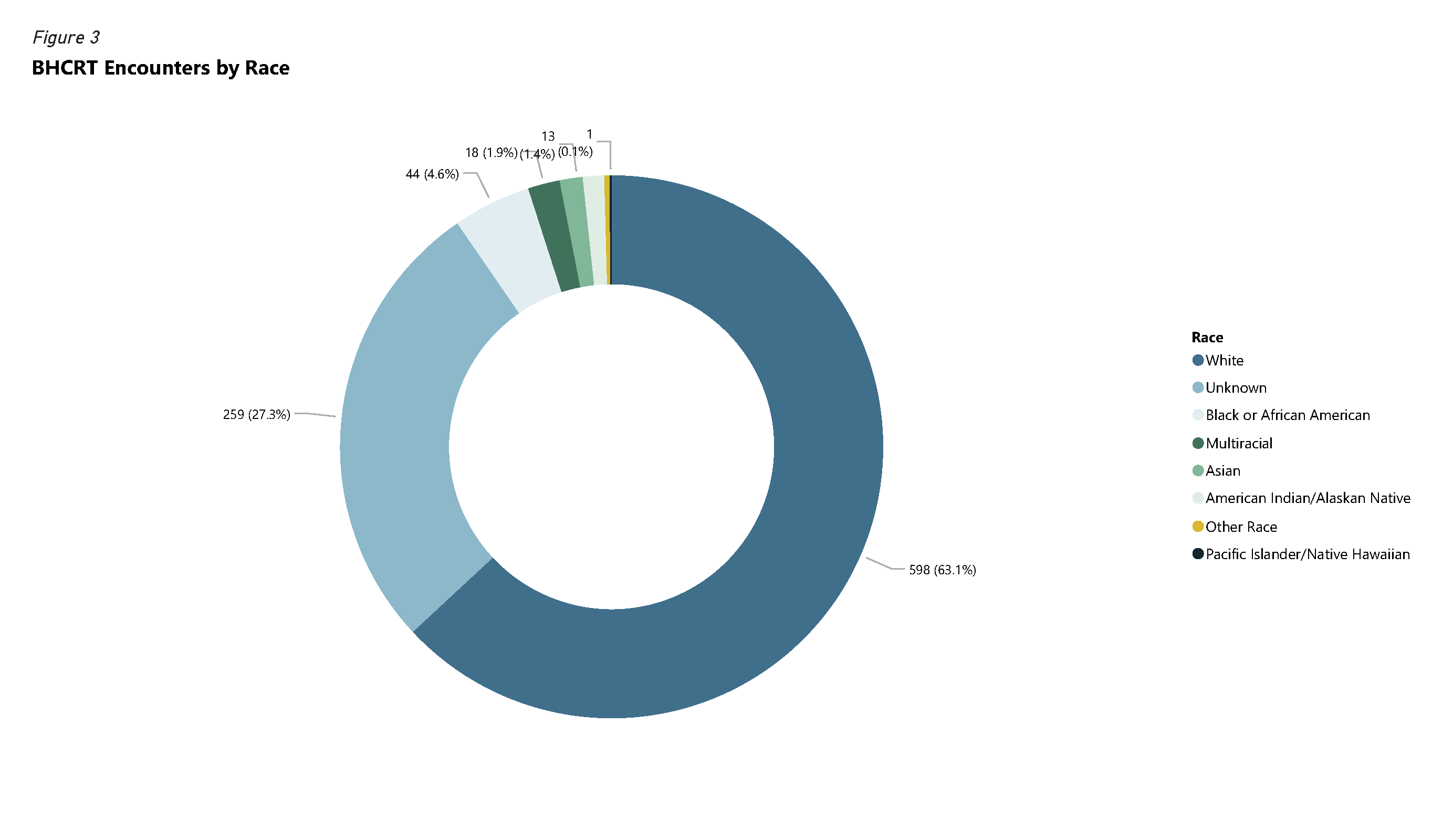
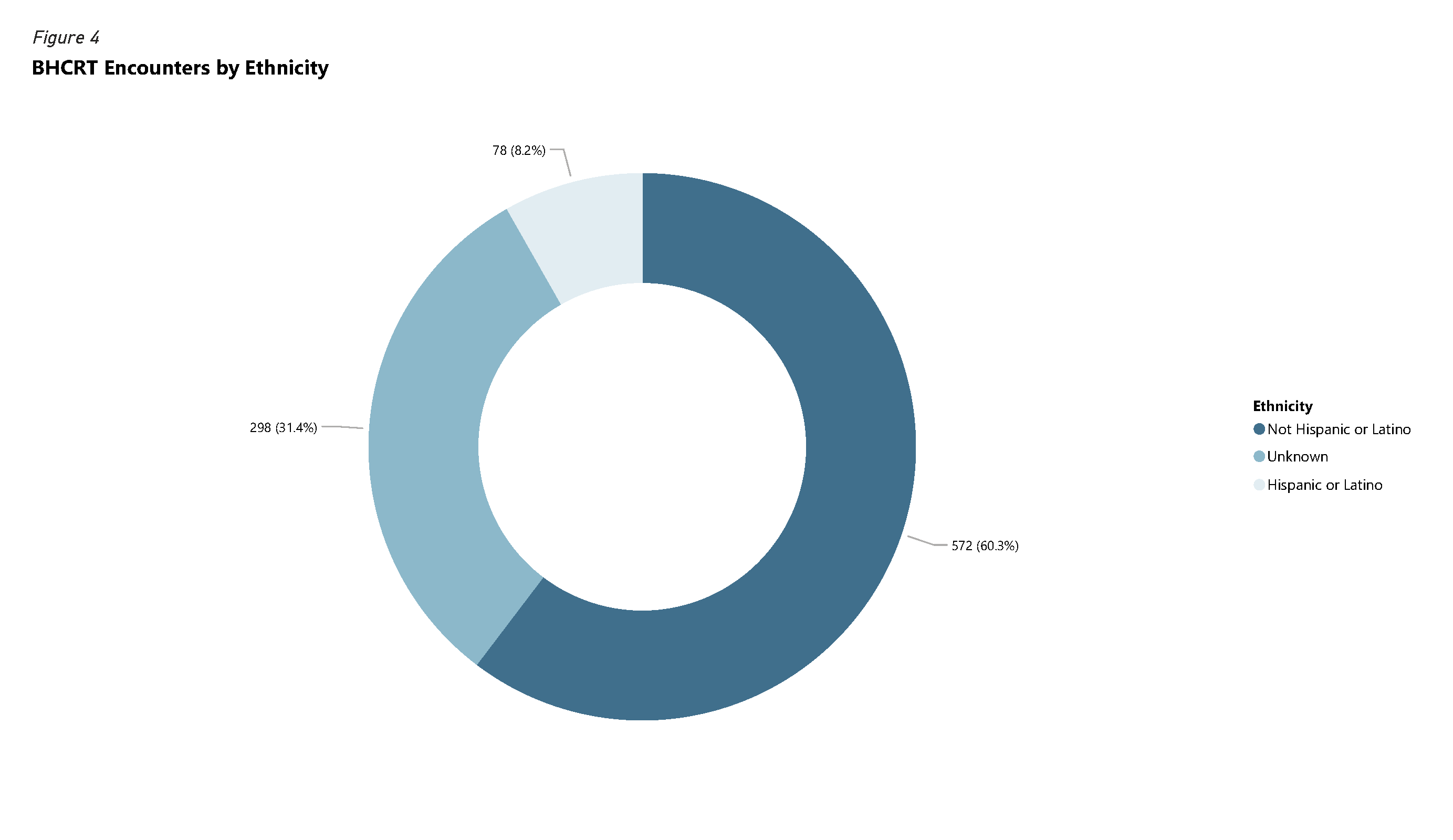
Race and Ethnicity
Race and ethnicity are typically self-reported by clients as BHCRT staff do not necessarily know how an individual identifies. This results in limited reporting of this demographic category, particularly since crisis situations are not always conducive to discussions about race/ethnicity. Figures 3 and 4 show available race/ethnicity data for 2025 in further detail.
Figure 3: BHCRT Encounters by Race
Of the 948 unique clients who reported their race; 63.1% identified as White, 4.6% as Black or African American, 1.9% as multiracial, 1.4% as Asian and 27.3% were unknown. Less than 1% of clients identified as American Indian/Alaskan Native, Pacific Island/Native Hawaiian, or Other Race.
Figure 4: BHCRT Encounters by Ethnicity
Housing Status
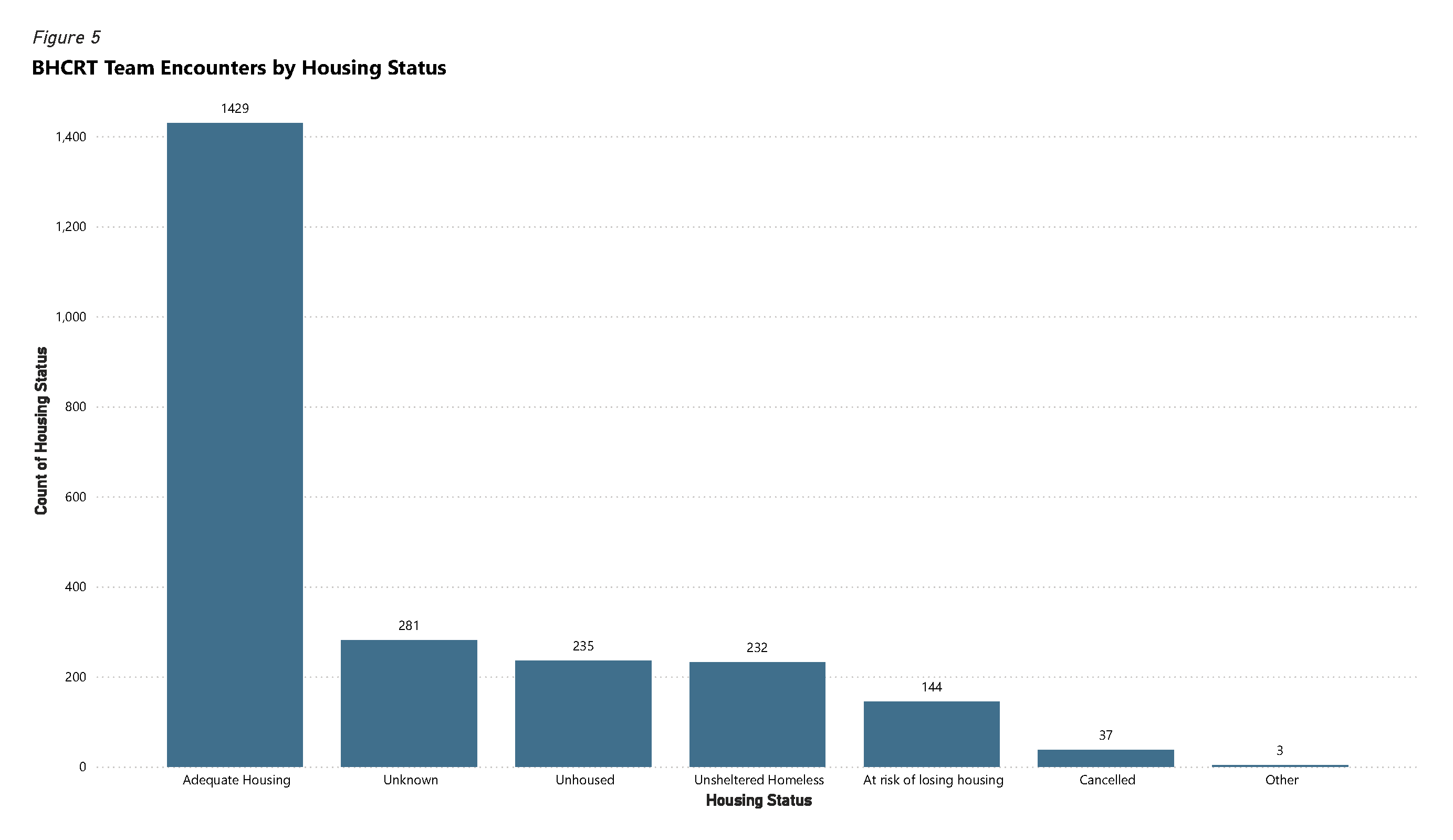
Most BHCRT clients have some form of housing in the community. 1 in 5 BHCRT responses involved someone without housing, indicating that unhoused community members, who make up less than 1% of the City’s population, are over-represented in crisis response. An additional 6.1% of BHCRT encounters involved people at risk of losing housing. The clinicians on the team have observed some relationships between behavioral health crisis and loss of housing, as behavioral health crisis can impact housing stability and vice versa. In cases where individuals were seen multiple times by BHCRT in 2025, housing status was recorded each time, reflecting 2,361 housing status entries for 951 unique individuals which can be seen in Figure 5.2
People who are living in a shelter, motel or vehicle are considered unhoused. An individual experiencing unsheltered homelessness is a person living in a place that is not meant for human habitation; such as living in a tent, on the streets, in their vehicle, or in an RV without access to basic necessities (e.g., water, heat, toilet, shower).
Figure 5: BHCRT Encounters by Housing Status
People with Multiple BHCRT Calls for Service
27.1%, or 222 of 819 unique clients, had more than 1 encounter with the BHCRT in 2025.
The 10 clients with the highest number of BHCRT calls for service interacted with BHCRT an average of 14.8 times in 2025.
The BHCRT works with clients, as well as a wide variety of related community service providers, to connect people with ongoing community support. However, some individuals have a combination of serious mental health and substance use issues that make it difficult to consistently engage in non-emergency care. In addition, care for certain conditions – such as methamphetamine use – is limited and not easy to access for all populations. Finally, it can be difficult for people without stable housing to engage in mental health treatment or substance use recovery because the basic need for safety, food and housing will typically overshadow other needs.
Response Trends
The BHCRT responds when dispatched by Police and Fire Communications or requested by a police officer. The BHCRT can also assign themselves to calls in instances where they are familiar with the person involved or otherwise recognize that there is a behavioral health component.
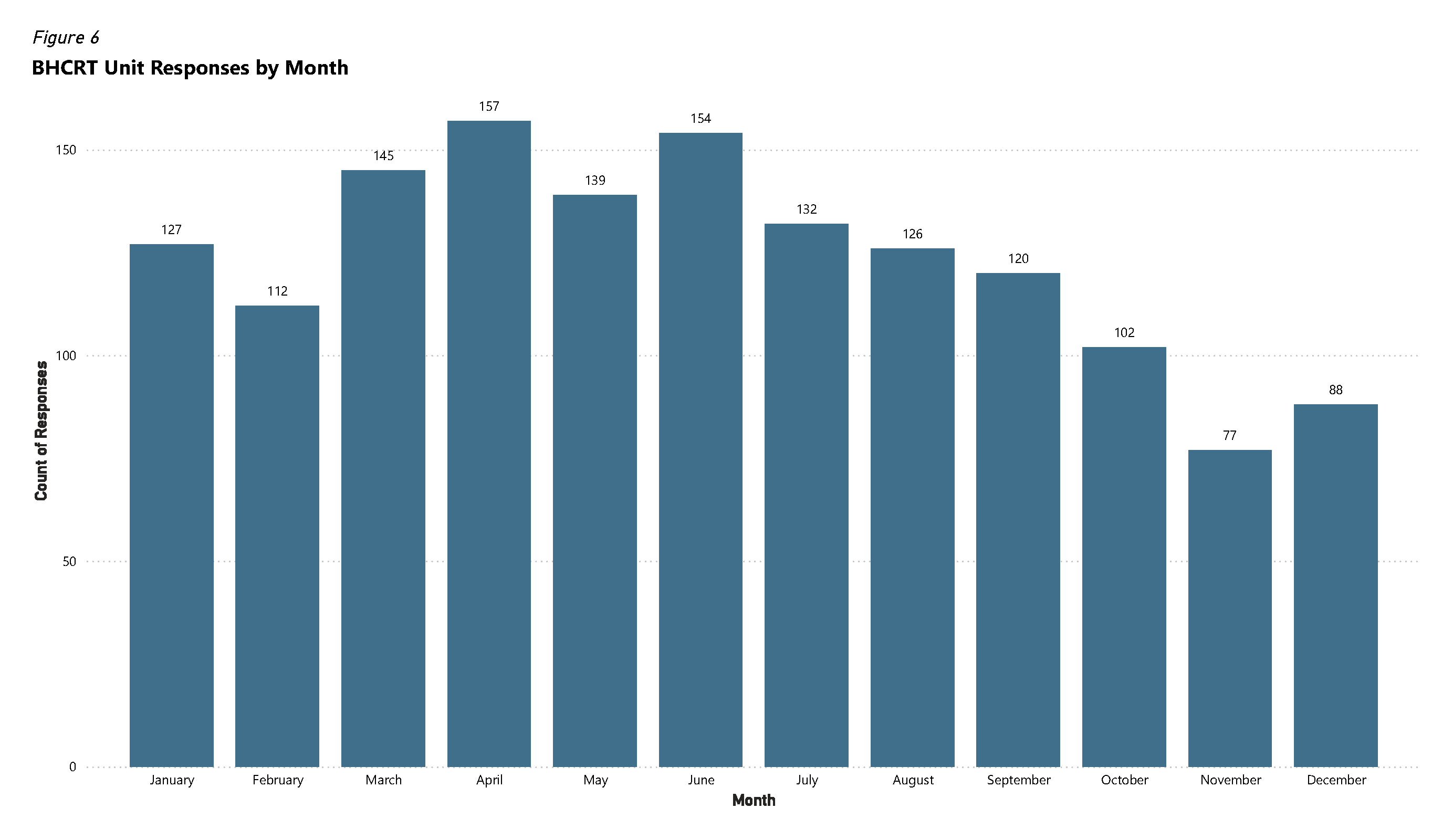
The team responded to 1,479 calls for service during 2025. This number does not include follow up calls made by the team after initial contact. The team had 166 fewer responses in 2025 than in 2024 which may be partially due to clinician vacancies during the last four months of 2025.
Figure 6: BHCRT Unit Responses by Month
Follow Ups
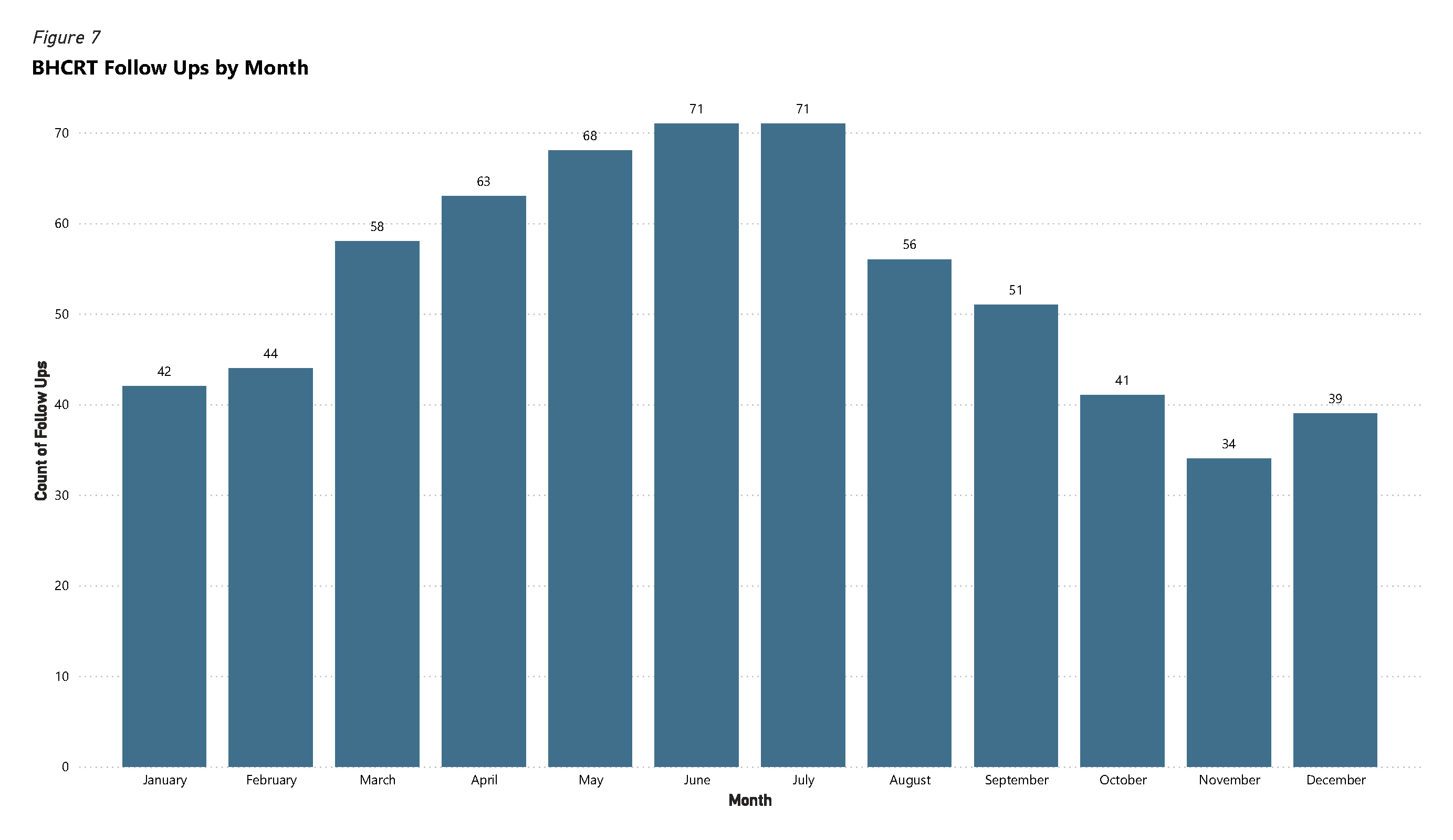
Follow up notes are used by clinicians to document follow up interactions. Common examples include a clinician following up with a client after a call for service (e.g., via phone or in person) or a clinician responding to a voice mail message that was left on the team phone line.
Figure 7: BHCRT Follow Ups by Month
Information Notes
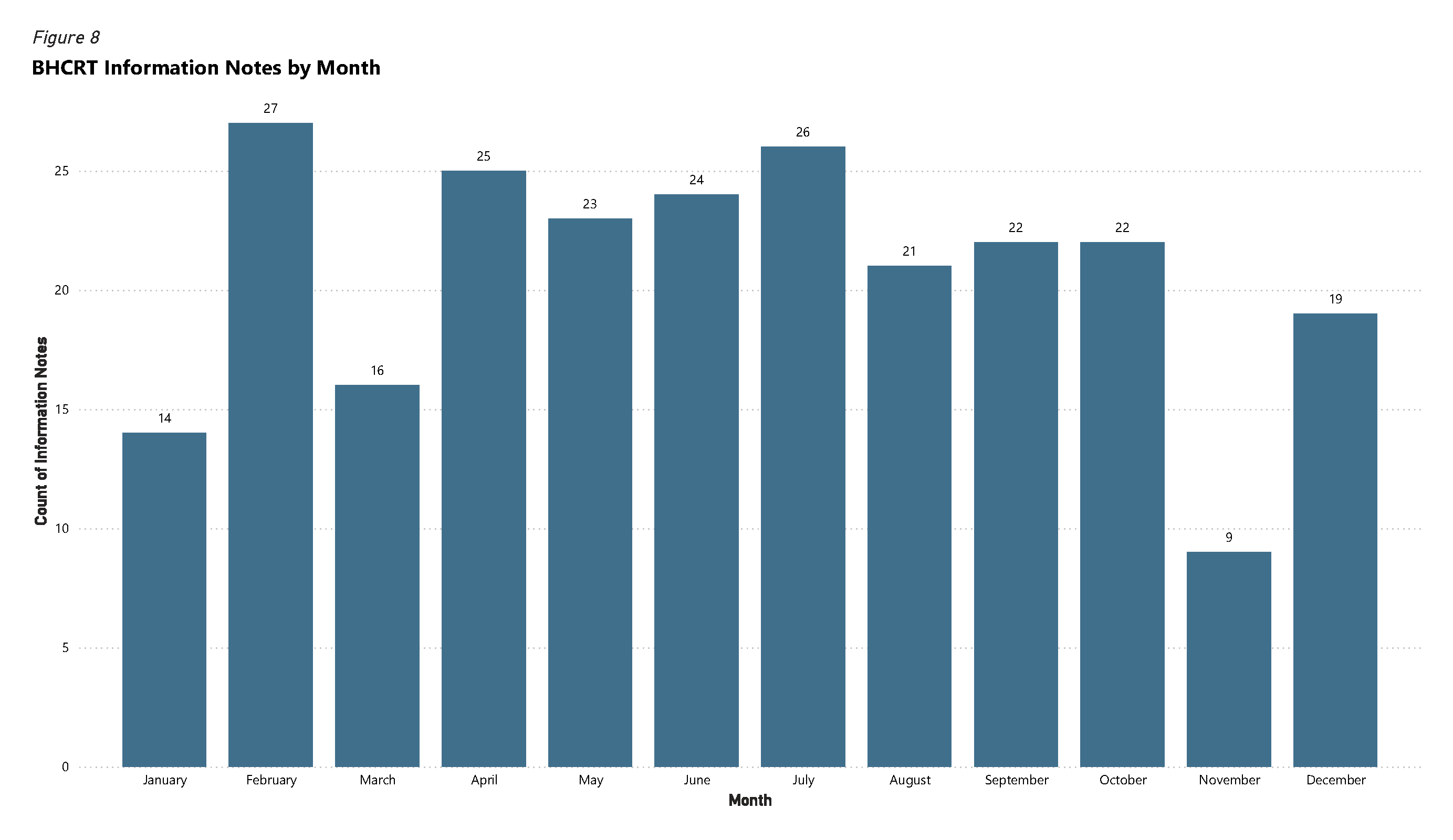
Information notes are created by clinicians when they receive clinically relevant information from a third party about someone in the community and that information does not require an immediate response or follow up. An example of when this note type would be used is when a police officer sends an email with information about an individual in case the BHCRT comes into contact with them in the future, but there is no current need for the person to be contacted.
Figure 8: BHCRT Information Notes by Month
Call Volume: Time of Day, Day of Week
The BHCRT seeks to align service with highest volume times for behavioral health calls.
The BHCRT service hours through August 2025 were:
Monday through Friday from 8 a.m. to 11 p.m.
Saturday through Sunday from 9 a.m. to 9 p.m.
Hours were reduced for the last four months of 2025 due to staff vacancies.
Figure 9 displays the total number of calls during each hour of different days of the week in 2025 when analysis of key words in dispatch data indicates the call may have been appropriate for BHCRT response.
Overall, BHCRT hours match well with high volume times for crisis calls to Boulder Police and Fire Communications.
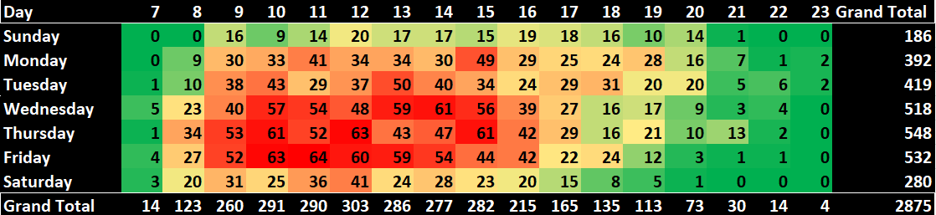
Figure 10 demonstrates the number of calls BHCRT responded to by hour of day and day of week during 2025. There are several reasons for the difference between the 10,207 calls considered appropriate for BHCRT response, and the 2,8753 calls responded to by BHCRT.
At times, BHCRT clinicians were unable to go to calls if they were already assigned to another call.
There were 10,207 total calls that may have been appropriate for the BHCRT in 2025 based on keywords in dispatch’s Computer Aided Dispatch (CAD) system. 2,471 calls matching key words for BHCRT response fell outside of planned BHCRT hours (24.2%). This means an average of approximately 6.8 calls per day fell outside regular BHCRT hours.
Figure 9: BHCRT Unit Demand by Day of the Week and Hour of the Day
Figure 104: BHCRT Unit Responses by Day of the Week and Hour of the Day
Primary Concerns – Types of Issues Faced by Community Members Interacting with BHCRT
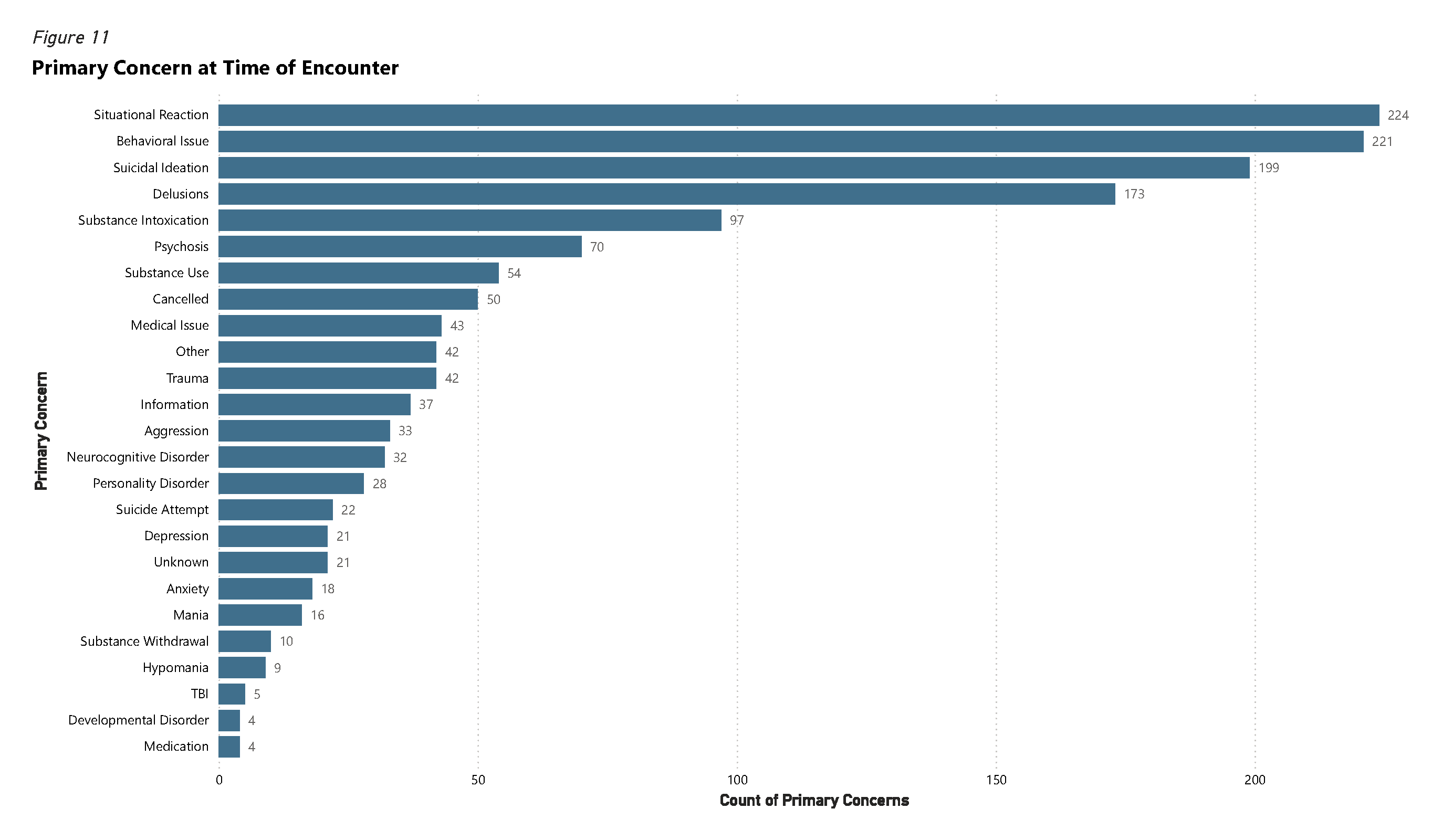
Community members seek assistance for a wide variety of behavioral health situations, with some people experiencing multiple concerns. Most common primary concerns in 2025 included Situational Reactions and Behavioral Issues.
Situational Reactions are circumstances where the person’s behavior is driven by a reaction to a specific situational stressor rather than a mental illness or substance intoxication. Examples include a relationship breakup, failing a test or being fired from a job. Situational reactions are often paired with underlying issues that make people more vulnerable to behavioral or emotional dysregulation such that external events precipitate a crisis reaction.
Behavioral Issues describe issues with behaviors that are disruptive or otherwise incompatible with the person’s current environment. This could be someone having difficulty regulating following an upsetting event, someone who used drugs or alcohol and then behaved in a way that created issues beyond simply being intoxicated, or someone having an outburst related to rules or boundary setting.
224 clients, 15.1% of encounters, had a primary concern related to Situational Reactions and another 221 clients, 14.9% of encounters, had a primary concern related to Behavioral Issues in 2025. The least frequently cited concerns for BHCRT encounters were Developmental Disorder (0.3%) and Medication (0.3%).
Figure 11: Primary Concern at Time of Encounter
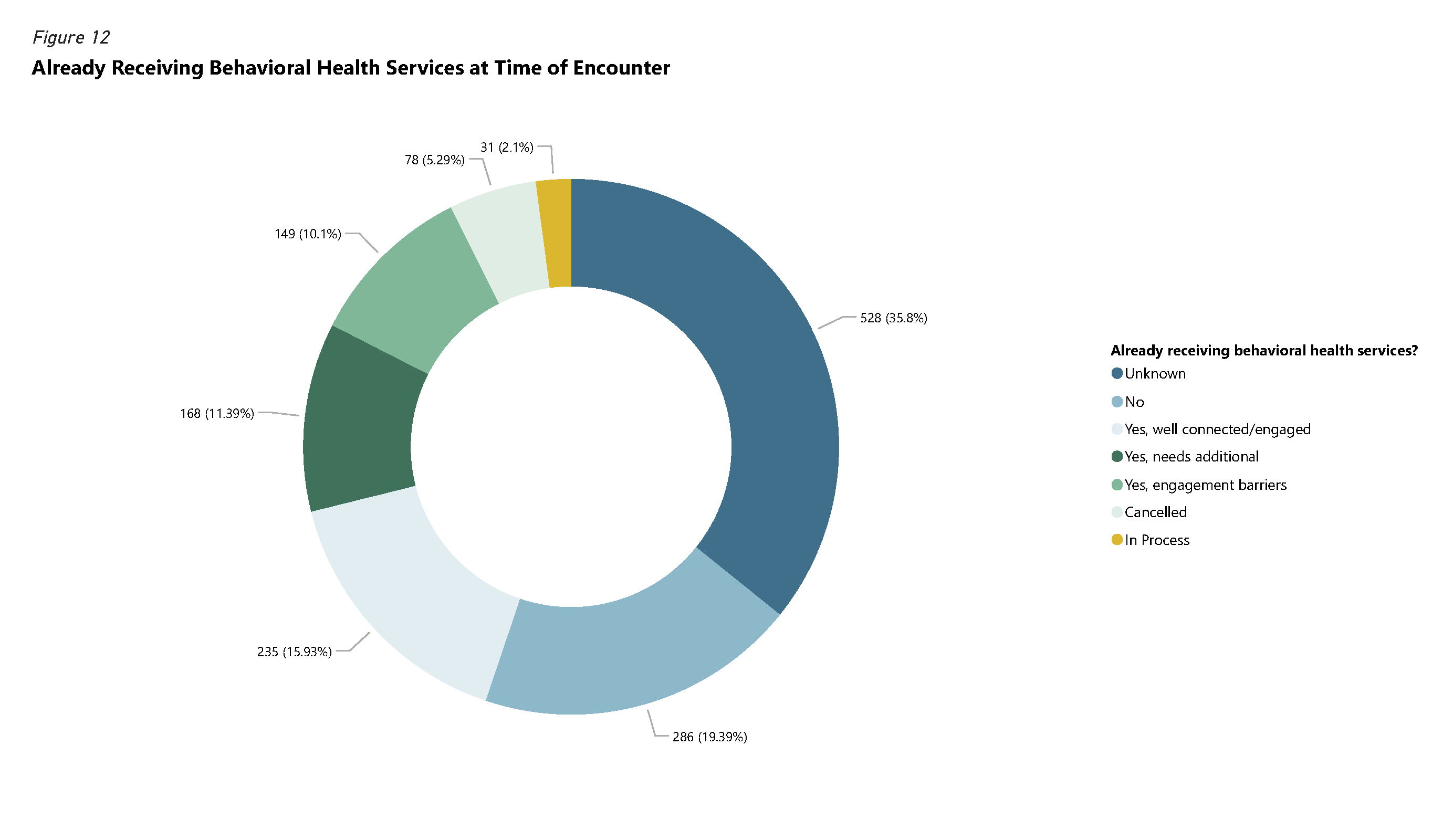
Current Care Status
552 (37.3%) non-unique clients5 interacting with BHCRT reported that they were already receiving behavioral health services from a provider; 286 (19.3%) clients reported not receiving any behavioral health services; 31 (2.1%) reported being in the process of obtaining behavioral health services.
Figure 12: Already Receiving Behavioral Health Services at Time of Encounter
Outcomes
Referrals
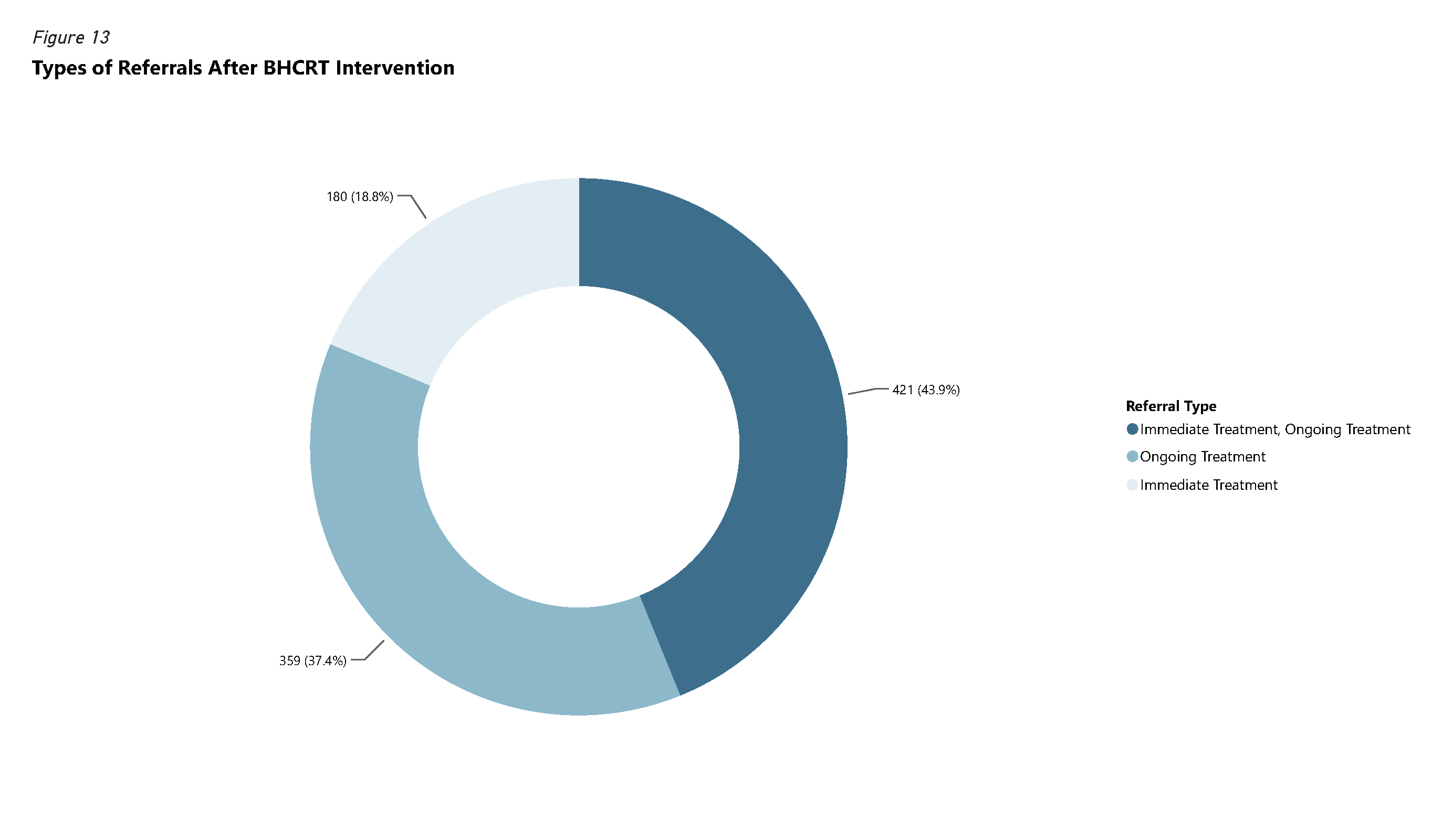
Clients are referred to a variety of community resources and ongoing treatment options. In some cases, people have an immediate need for further treatment. Immediate treatment includes being transported to a hospital emergency department or accessing the walk-in crisis clinic or detoxification facilities operated by Clinica Family Health & Wellness.
The team also tries to connect people with ongoing community treatment and other support resources (e.g. food banks, homeless services, etc.). Many referrals are done as part of follow up calls because people are not always able to engage in conversations about follow up care while experiencing a behavioral health crisis. In some cases, people do not wish to participate in follow up discussions or cannot be reached for a follow up. Figure 13 displays the distribution of referrals where this data is available for BHCRT contacts.
Figure 13: Types of Referrals After BHCRT Intervention
Mental Health Holds
BHCRT clinicians initiated emergency mental health holds 43 times (2.9% of calls) in 2025. An emergency mental health hold is a process where someone can be detained for up to 72 hours if they meet certain criteria due to a mental illness. The emergency mental health hold is an important mechanism to connect people with care during situations where they are at risk of serious harm and their symptoms are too severe to be managed on an outpatient basis. BHCRT clinicians weigh the decision to initiate mental health holds carefully, given that involuntary treatment can be helpful in some situations but harmful in others. One of the benefits of BHCRT clinical expertise on behavioral health calls is the reduction of involuntary treatment.
While involuntary treatment has a place in the continuum of care, it can have significant negative impacts. This may include decreased trust in care providers; trauma from being confined, restrained and medicated against one’s will; the financial burden of ambulance transport and inpatient treatment; disruption to relationships, education and employment; as well as the stigma of being placed on a mental health hold and being taken to the hospital.
Emergency Commitments
An Emergency Commitment is a process for involuntary treatment if someone meets certain criteria due to their use of alcohol or substances. People are usually taken to an emergency department or a detoxification facility and released once they are sober.
Use of Force and Arrests
Of the 1,479 BHCRT calls for service the team responded to in 2025, four (0.3%) involved use of force by an officer. One use of force occurred when an officer used their TASER on a person who was holding a weapon and threatening another person with it. One was a TASER display. In another incident, an officer had his rifle slung when responding to a call about a domestic dispute where one party had a firearm. The fourth use of force happened on a call where a person took out a knife during a call for a disturbance and began moving towards officers. The officers displayed their firearms, and the person put the knife down. BHCRT was physically present during one of these incidents; the others happened prior to the team’s arrival.
23 (1.6%) of BHCRT’s calls for service in 2025 involved an arrest. 13 arrests involved the subject having a warrant, violating a protection order, assaulting or menacing someone, or abusing a child. Six other arrests involved a mixture of charges (harassment, obstruction, drug possession, criminal mischief, tampering), with the common denominator being some form of trespassing. Two arrests were made by outside jurisdictions, and we do not have further information. One was for driving under the influence and driving under restraint while one was for possession of a weapon on school grounds.
Remaining in the Community
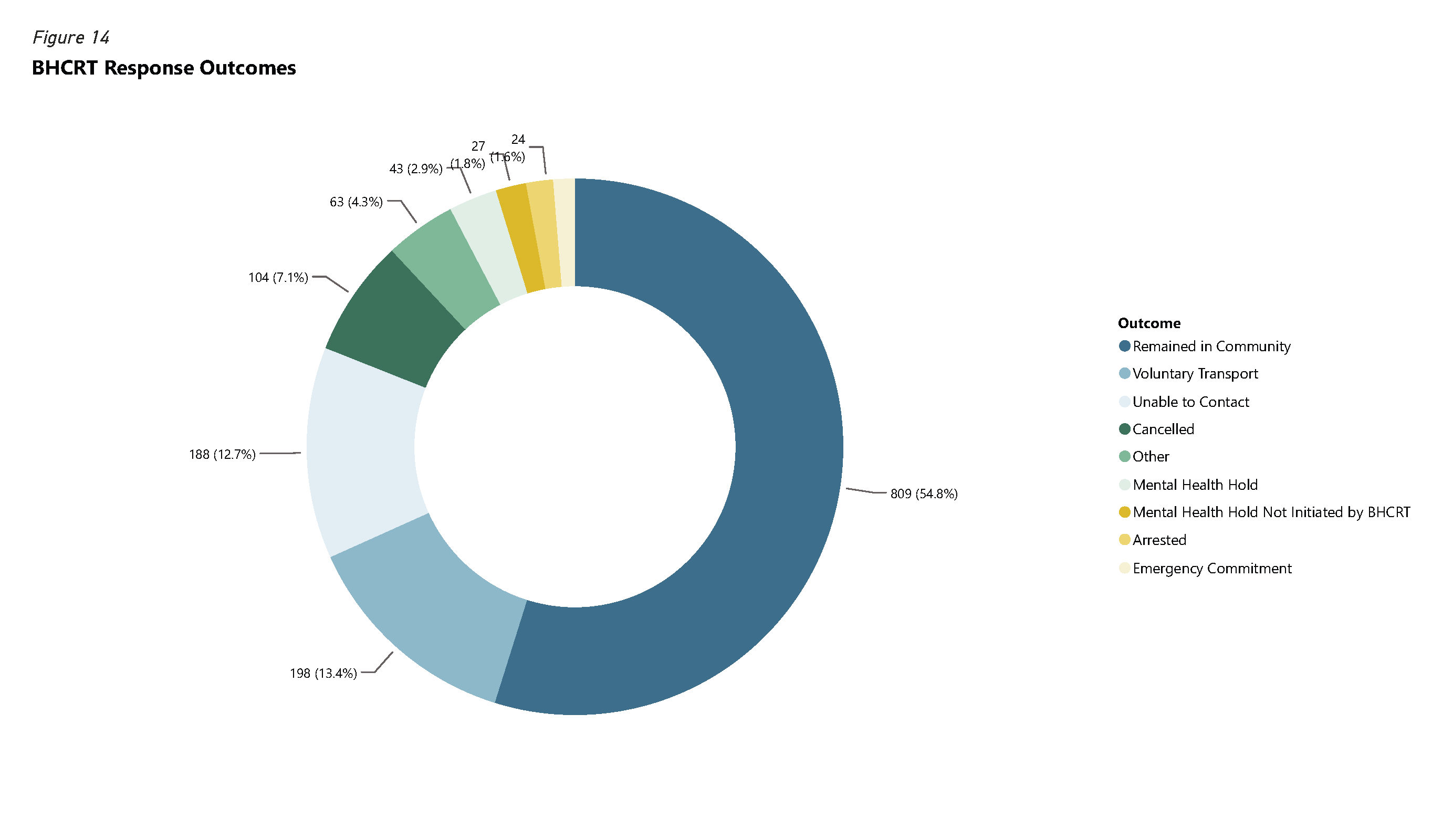
The preferred outcome in mental/behavioral health crisis response is typically for the community member to remain in the community. That means the situation was able to be resolved without someone going to a higher level of care. Remaining in the community has several advantages over hospital stays including providing care in a less disruptive manner, improved recovery rates, easier access to support networks, lower health care costs and reduction of stigma. 68.4% of BHCRT calls for service in 2025 ended with the client remaining in the community.
Figure 14: BHCRT Response Outcomes
Facilitating Return of First Responders to Service
One goal of the BHCRT program is to facilitate a response that meets the needs of the community. One of the ways the team supports this goal is by clearing first responders from calls that BHCRT is on so those first responders can be available to go to other emergencies.
A facilitated return of Fire/EMS to service indicates that the clinician on the call was able to clear Fire/EMS from the call and return them to service, allowing them to respond to other calls for service. If the clinician was unable to return Fire/EMS to service this indicates that Fire/EMS stayed on the scene through the completion of the call. BHCRT facilitated return of Fire/EMS to service 170 times (40.3% of applicable interactions).
A facilitated return of law enforcement to service indicates that the clinician was able to address a contact that otherwise would have been assigned to an officer, or the clinician was able to clear one or all officers assigned to the call for service from the scene. If the clinician was unable to return law enforcement to service this indicates that officers remained on the scene for the duration of the contact. BHCRT facilitated return of police to service 515 times (45.7% of applicable interactions).
Case Management
An essential part of the crisis response program is connecting people with ongoing services in the community. Most of this connection work is done by the team’s case managers following a crisis.
Case managers handled referrals for 174 clients in 2025. Fifty-seven of these clients utilized resource navigation services, twenty-five engaged in active case management, and ninety-two were referred to case management but chose not to work with the case management team. Clients engaged with case management had an average of 4.2 interactions per client throughout the year.
Case Management Referrals
Case management consists of resource navigation, where people are directed toward resources, and more intense active case management.
Resource navigation is for people who are able to access services with minimal support. These clients may be able to meet their needs using existing services but could use some support in redirection or problem-solving during a period of crisis. Resource navigation clients may also not want more active case management but will accept resource navigation.
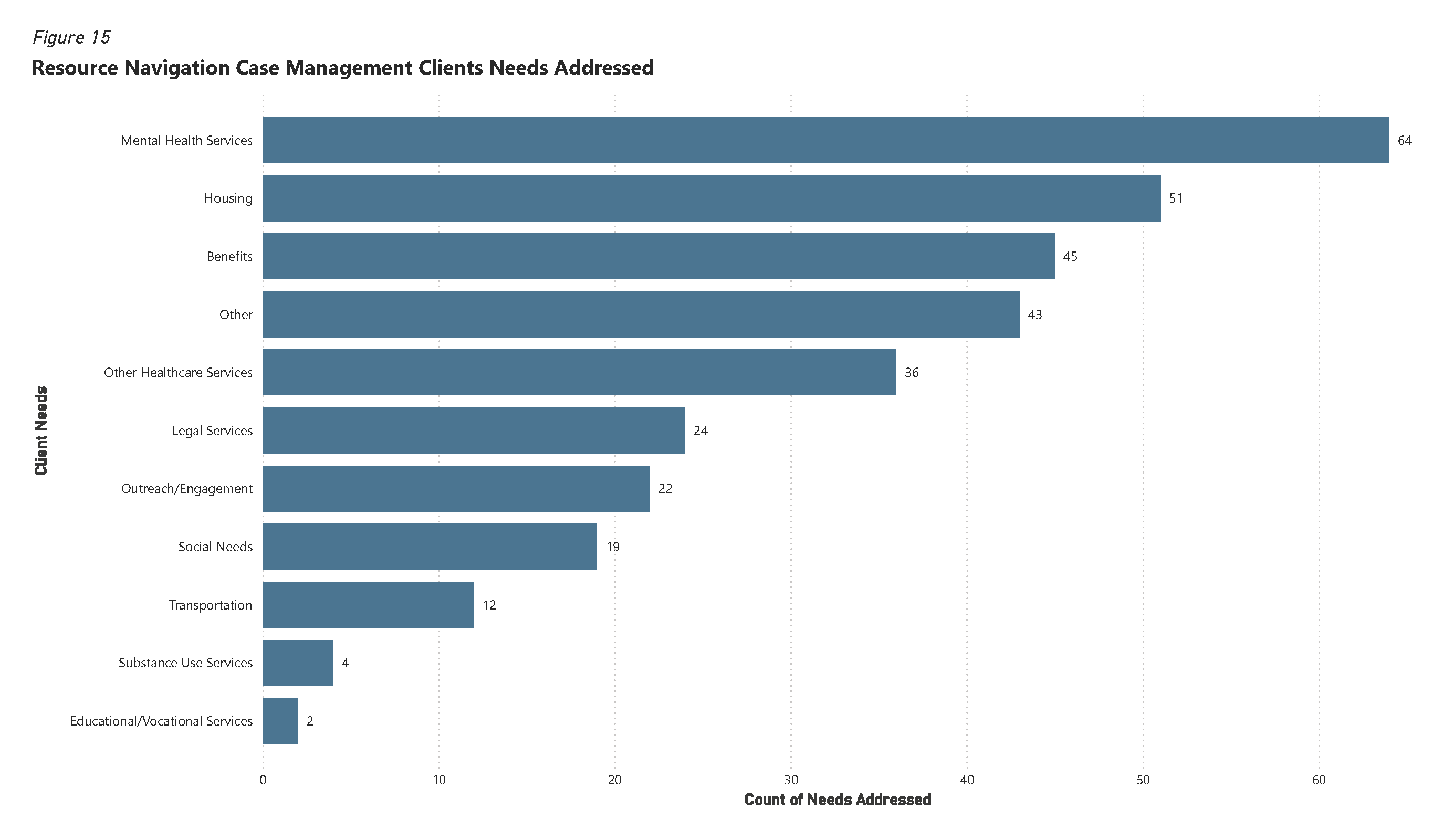
Figure 15: Resource Navigation Case Management Clients Needs Addressed
There were 322 needs addressed by case managers with resource navigation clients. The most common needs addressed by resource navigation were mental health services (19.9%), housing (15.8%) and benefits (14.0%). Figure 15 shows the number of resource navigation sessions that addressed each need. More than one need can be addressed in a session. Fifty-seven people received resource navigation services during 2025.
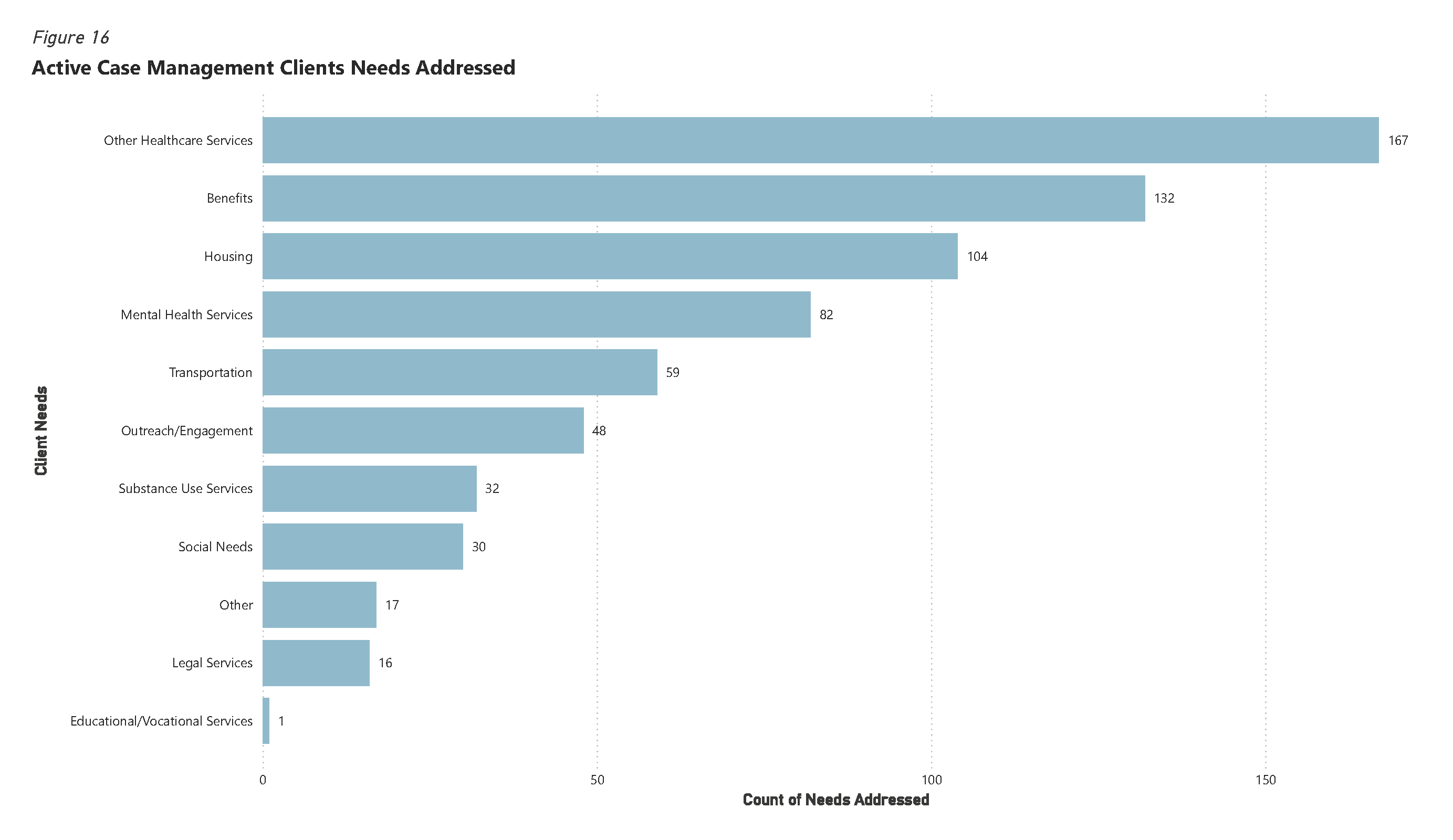
Figure 16: Active Case Management Clients Needs Addressed
Active case management clients receive more intensive coordination of services, typically over a longer time period. Case managers enroll clients into active case management when clients need more support to connect with service providers in the community and address their goals. Case managers meet with clients as often as needed.
Twenty-five people received these services over 352 interactions; some of these people also received resource navigation. The needs addressed for active case management clients were different from those of resource navigation clients. Other health services (24.3%), benefits (19.2%) and housing (15.1%) were the most common needs addressed for active clients.
Case Management Demographics
The case management team assists a wide variety of people in the City of Boulder.
Age
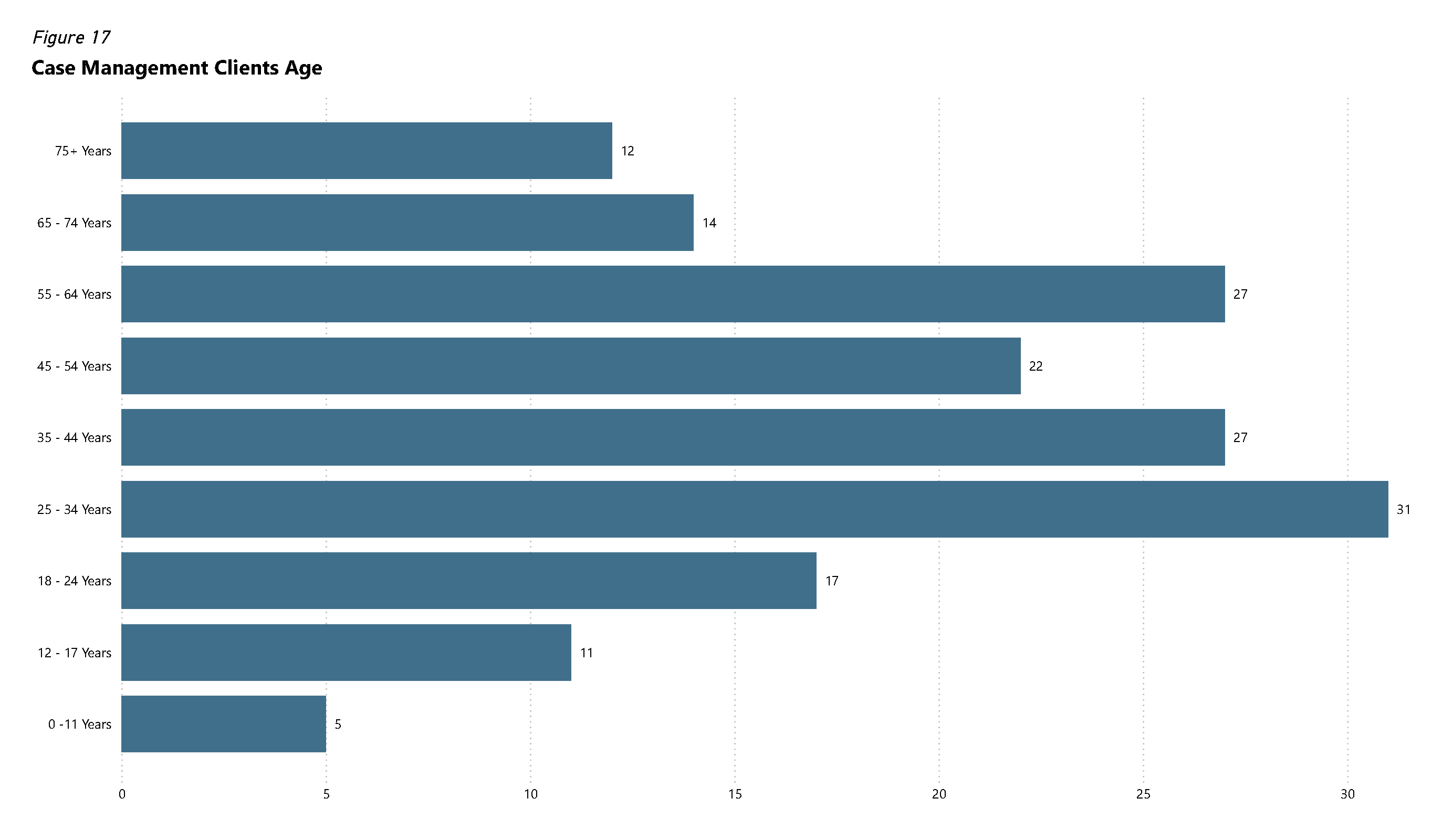
The median age of case management clients during 2025 was 43 years old, with a range from 6 to 88 years old.
Figure 17: Case Management Clients Age
Gender
Of the 174 clients who reported their gender, roughly 50.0% identified as male, 47.1% as female, 1.7% as transgender, and 0.6% as non-binary.
Race and Ethnicity
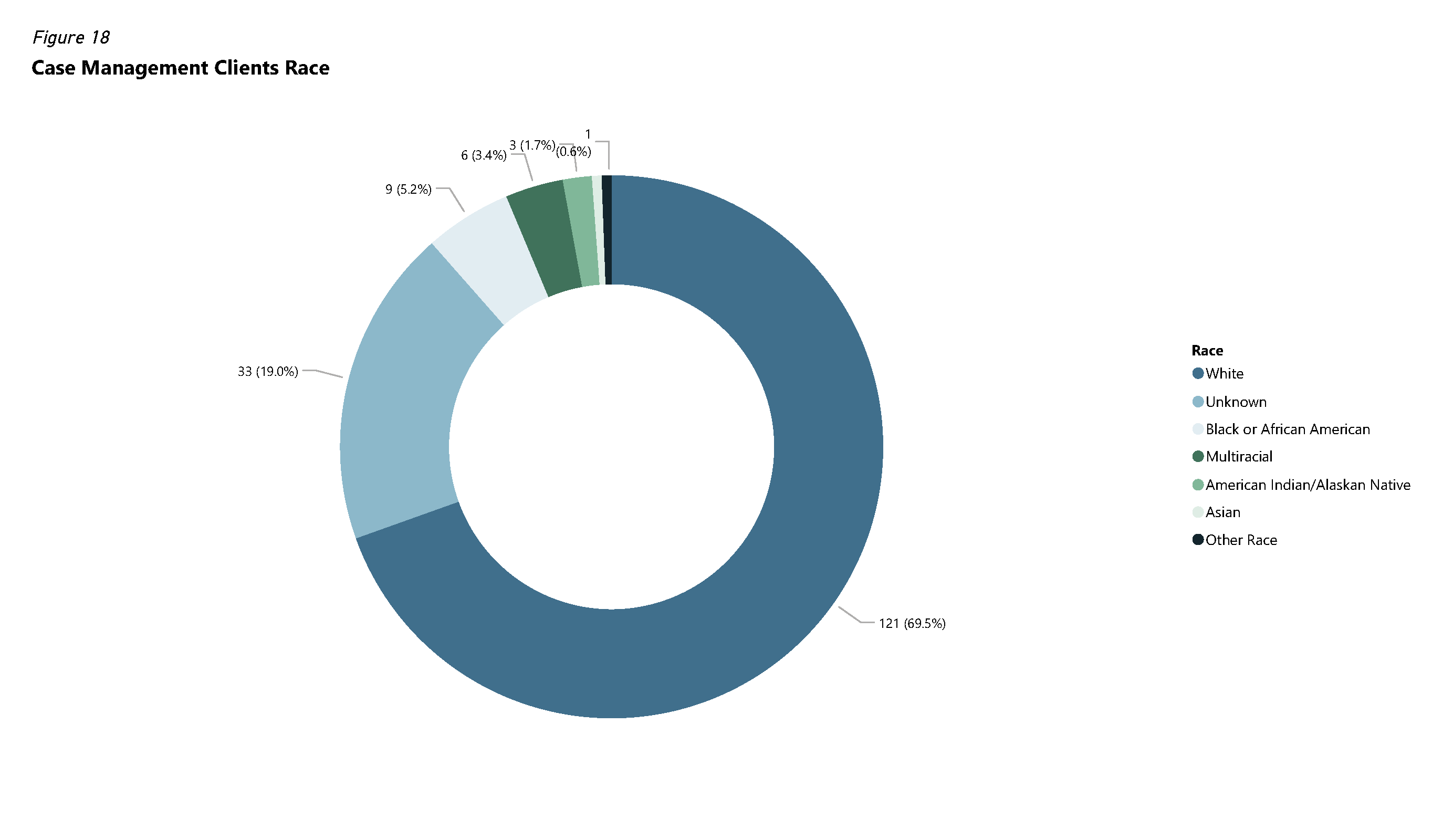
Of the 948 unique clients who reported their race, 69.5% identified as White, 5.2% as Black or African American, 3.4% as multiracial, and 19.0% were unknown. Less than 1% of clients identified as Asian, American Indian/Alaskan Native, or Other Race.
Figure 18: Case Management Clients Race
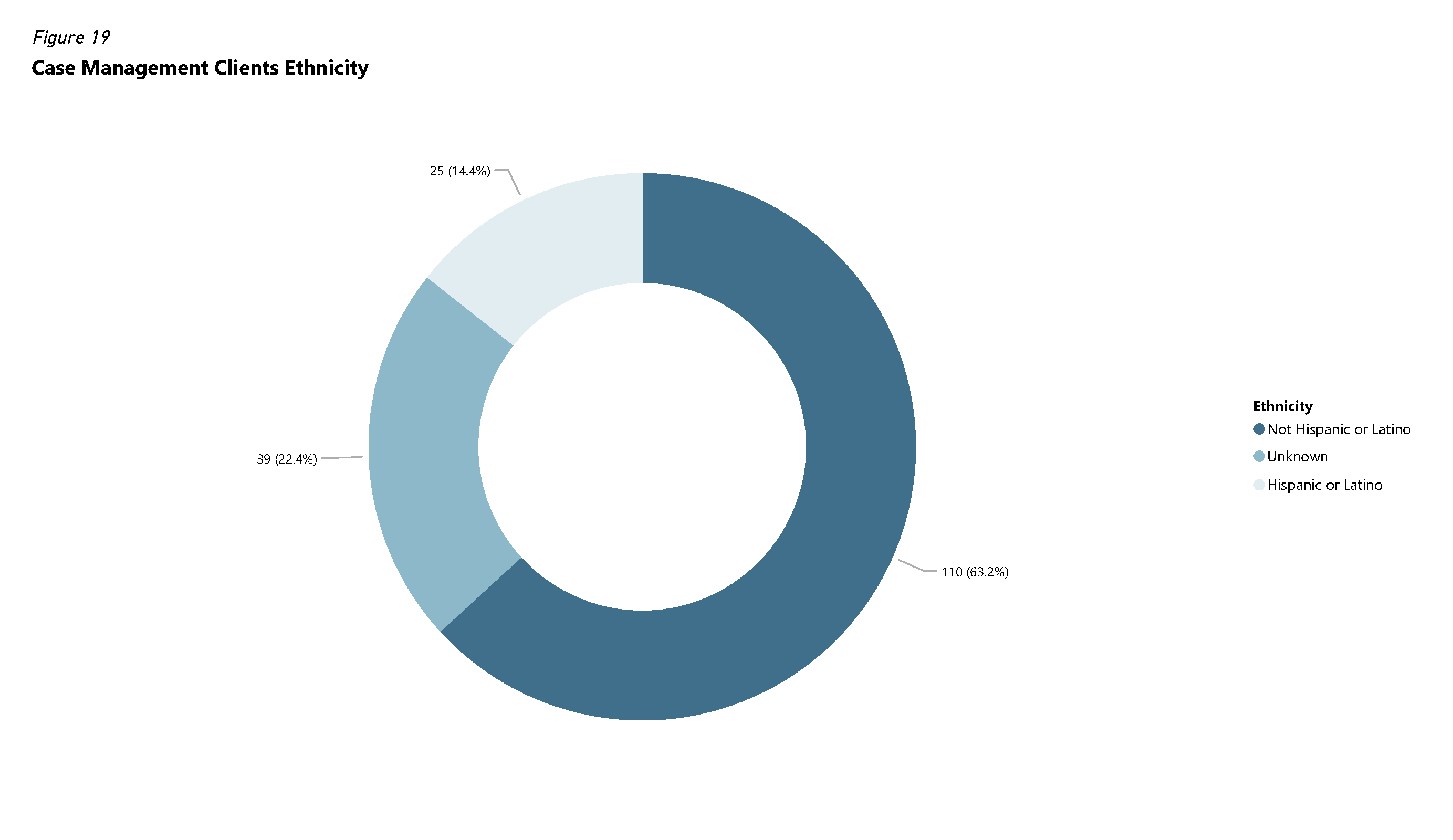
Figure 19: Case Management Clients Ethnicity
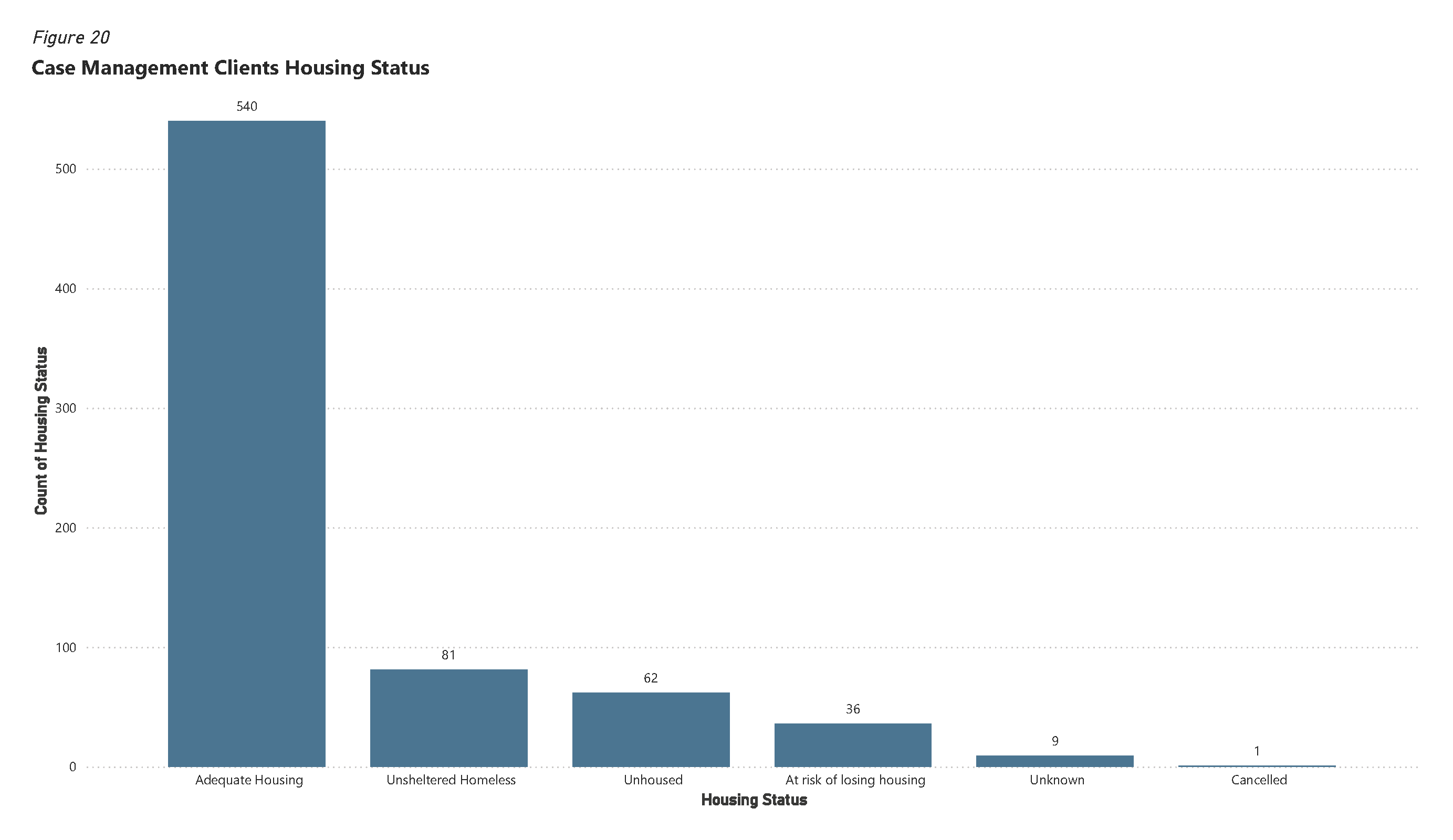
Housing
Figure 20: Case Management Clients Housing Status
Footnotes
In the third quarter of 2025, the Crisis Intervention Response Team (CIRT) was combined with the former Community Assistance Response and Engagement (CARE) team, to form the current Behavioral Health Crisis Response Team (BHCRT). This report includes the combined activities of CIRT and CARE in 2025.
A client’s housing status may change over time due to various factors. To represent these potential changes the housing status for all interactions are shown in Figure 5 instead of by unique client as is the case with the other demographic figures.
The 1,479 BHCRT responses recorded in CAD includes BHCRT calls for services, BHCRT follow ups, and BHCRT case management follow ups. Some follow ups completed by the team do not appear in CAD because they are not calls in the emergency system. Therefore, some numbers in this section appear different than response and follow up numbers included earlier in the report.
Figure ten includes duplicate calls for service, which is why the grand total included in the graphic is 2,875. With duplicates and canceled calls removed, the total number of unit responses recorded by BPD was 1,479. These responses include BHCRT calls for service and follow ups.
Current care status can change over time. For this reason, non-unique clients were used for this metric.